ICSR Validation and Minimum Criteria in PV | PVCON Consulting
Learn how PV teams misinterpret ICSR minimum criteria, misclassify incomplete cases as invalid, and silently lose reportable cases through weak follow-up and documentation.

ICSR Validation: How Teams Misinterpret Minimum Criteria and Silently Lose Reportable Cases
The message often sounds harmless:
"Doesn't meet minimum criteria. Not reportable, right?"
That is where the risk begins.
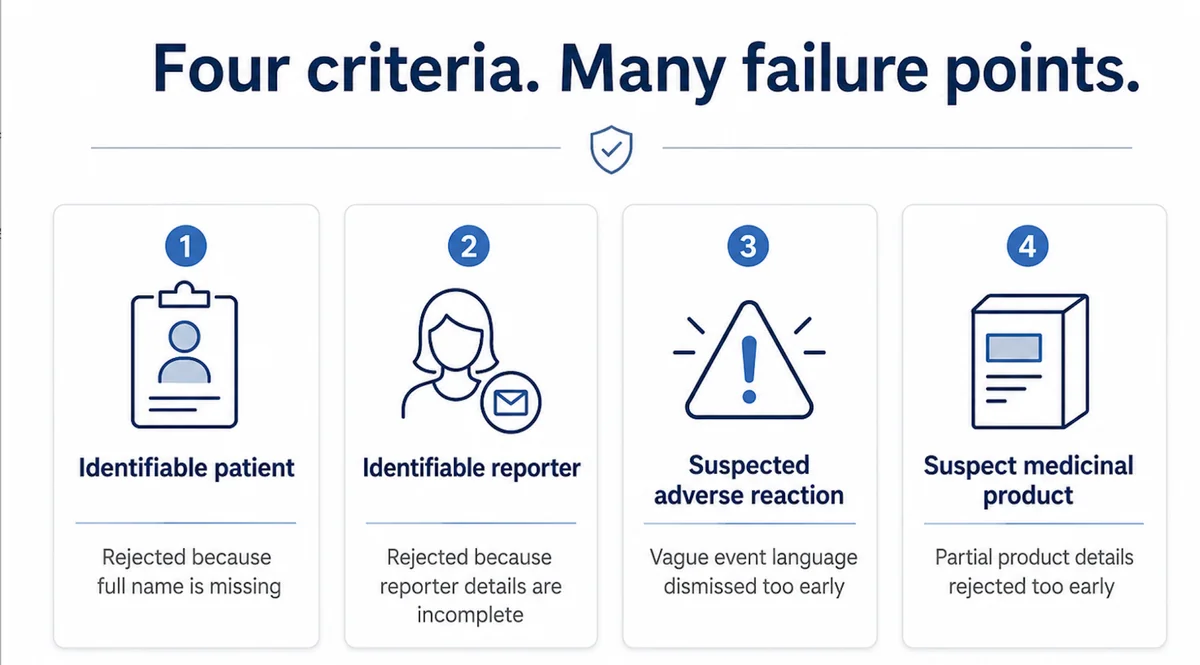
A valid ICSR needs four minimum criteria: an identifiable patient, an identifiable reporter, a suspected adverse reaction, and a suspect medicinal product. But when teams use these criteria as a rejection filter, weak or incomplete reports may be closed too early.
Follow-up is missed. The rationale is not documented. The case never reaches reportability assessment.
Recent regulatory enforcement has shown that the issue is not only late reporting. It is also how minimum criteria and invalidity decisions are applied before a case reaches proper assessment.
Minimum Criteria Are Not a Rejection Shortcut
Minimum criteria help decide whether a case is valid for further processing and potential reporting. They should not be used to close unclear reports too early.
An incomplete case should trigger documented assessment and follow-up where possible, not automatic invalidation.
The better question is:
Can this report reasonably be clarified, validated, upgraded, or linked to a reportable safety case?
Once a case is closed as invalid, it may never appear in signal review, aggregate review, vendor quality checks, or inspection sampling unless someone specifically looks for it.
The Four Criteria Are Simple. Their Application Is Not.
| Minimum Criterion | Common Misinterpretation |
|---|---|
| Identifiable patient | Rejecting because full name is missing, even when age, sex, initials, or other details may identify the patient |
| Identifiable reporter | Rejecting because the reporter name is incomplete, even when contact details or source information exist |
| Suspected adverse reaction | Rejecting vague patient language instead of assessing the reported medical event |
| Suspect medicinal product | Rejecting partial product details too early instead of attempting clarification |
For example, "patient felt dizzy after taking the medicine" may not be medically complete, but it may still contain a patient, a reaction, and possible product exposure. It needs assessment, not automatic dismissal.
Incomplete Is Not the Same as Invalid
This is the key distinction.
- Incomplete case: A report is missing some information, but it may become valid after follow-up or clarification.
- Invalid case: The report does not meet minimum criteria after assessment and reasonable follow-up, and there is no basis to process it as a valid ICSR.
- Reportable case: A valid case that meets applicable reporting requirements based on seriousness, source, product, territory, expectedness, and local rules.
The mistake happens when teams jump from "incomplete" to "invalid" without documenting why.
That is not just a case processing issue. It is a quality system issue.
Causality and Weak Information Should Not Close the Door Too Early
One high-risk fallacy is treating weak causality or incomplete information as a reason to invalidate a case.
A report may have competing medical explanations, unclear timing, vague patient language, or a reporter who believes the event is unrelated. That does not automatically make it invalid.
The team should document the causality assessment, apply reportability rules, and trigger follow-up where possible. Uncertainty should not block the case from the safety system.
This matters across clinical trial reports, spontaneous reports, vendor call centers, product complaints, patient support programs, literature screening, and social or digital reports, where later information may validate or upgrade the case.
Why Silent Case Loss Matters Beyond Reporting Timelines
Misapplication of minimum criteria does more than create late reporting risk. It can affect the quality of the safety data pool.
When potentially valid cases are excluded before submission or signal review, recurring drug-event patterns may appear weaker than they are. This can affect signal detection, aggregate review, and benefit-risk evaluation.
The concern is not only one missed case. It is whether the process is systematically filtering out cases that should have been assessed further.
That is how a compliance gap remains silent.
What Inspectors May Check
Inspectors may review both submitted and non-submitted cases.
They may sample invalid case logs, non-reportable decisions, follow-up attempts, vendor scripts, product complaint screening records, upgrade timelines, seriousness and causality assessments, and literature or patient support program triage records.
The inspection question is not only:
"Was this case reported?"
It is also:
"Can the team justify why it was not reported?"
If invalidity decisions rely on memory, informal judgment, or missing follow-up evidence, the process is not defensible.
Practical ICSR Validation Checks
PV teams should regularly test how minimum criteria are applied.
Ask:
- Are incomplete cases followed up before closure?
- Are invalidity decisions documented with clear rationale?
- Are vendor intake teams trained on minimum criteria?
- Are product complaints screened for adverse event language?
- Are cases upgraded when new information becomes available?
- Are invalid and non-reportable logs reviewed for misclassification?
- Are borderline cases escalated for PV or medical review?
Quick test: pull a sample of recent invalid or non-reportable cases. If several were closed as "weak," "unclear," or "unlikely related" without documented follow-up and rationale, the validation process needs review.
How PVCON Consulting Supports ICSR Validation Readiness
ICSR validation is not just an intake task. It affects reporting compliance, signal detection, vendor oversight, inspection readiness, and PV system quality.
PVCON Consulting supports pharmaceutical, biotechnology, CRO, and medical device organizations through specialized services including GxP Audits, PV Audits, GCP Audits, Other GxP Audits, Pharmacovigilance Consulting, PV Quality Management System support, PvOIC services, Regulatory Intelligence, Medical Writing, Aggregate Report Writing, Clinical Safety Documents, RMP and REMS Writing, PSMF Management, and Training & Upskilling initiatives such as Training Matrix, Regulatory Compliance Training, PV Boot Camp, and Customized Learnings.
Our expertise helps organizations strengthen drug safety operations, improve inspection and audit readiness, and keep PSMF documentation compliant, accurate, and aligned with real-world PV system practices and regulatory expectations.
If you are evaluating your ICSR validation process or preparing for an inspection, you can contact our team or learn more about us.